During the last two decades, weight training has become very popular among the general population, in fact one in three Americans participates in activities related to weight training (1). This increase in the number of people doing this type of training has also increased the risk of soft tissue injury from overuse (2). Most of the injuries occur in the tendons because they are subjected to excessive stress or overload (2,3).
An area very prone to tendon injuries is the lateral aspect of the elbow (at the epicondyle, hence the name ” epicondylitis “), since many exercises with weights require grasping and / or pulling bars and / or dumbbells. These movements, with great weights and repeated over time (4), as well as an incorrect grip, can cause irritation of the musculootendinous tissues found on the lateral aspect of the elbow.
Below we will describe the injury, as well as the causes of it and the modifications that we must introduce in the training to minimize the risk of aggravating the injury and to be able to contribute to its recovery.
Description of the injury
Tennis elbow (epicondylitis) is characterized by pain in the lateral aspect of the elbow , and occurs in the dominant arm in 75% of cases (3). It is believed to be due to repeated movement in activities that require the forearm in pronation. Symptoms can last up to 24 months (5,6,7,8) and in 80% of cases they improve within a year regardless of the type of treatment (9). The number of cases with tennis elbow triples in people over 40 years of age who practice weight training or similar activities for two hours a day (2,10). It should be noted that the name of this injury is due to the fact that, according to various studies, between 40 and 50% of tennis players suffer this injury at some point in their sports career, with a prevalence between 5 and 9 times greater than suffering pain on the inside of the elbow (golfer’s elbow).
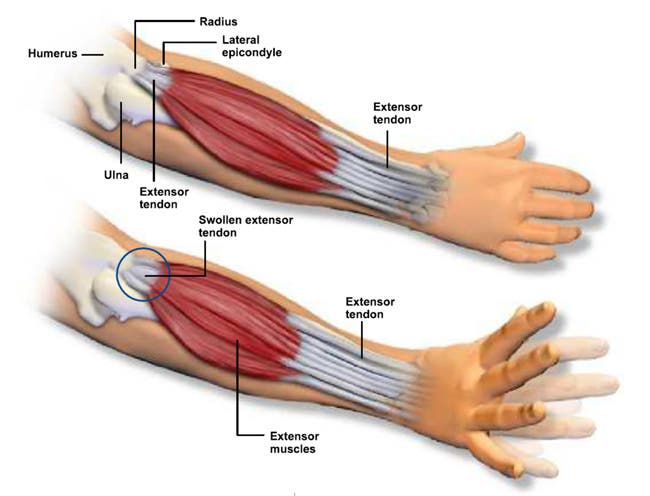
Regarding the anatomical disposition, we are not going to stop because you can get information about it in numerous web pages and books, and we do not want to enter into scientific terminology, so we are only going to list the different muscle tendon structures that can interfere with this injury :
- Elbow joint: humerus, ulna and radius.
- Extensor carpi radialis longus muscle.
- Extensor carpi radialis brevis muscle.
- Extensor carpi ulnaris muscle.
- Common extensor muscle of the fingers.
- Brachioradialis muscle.
- Long supinator muscle.
- Collateral ligament of the elbow.
- Annular ligament of the radius.
Terminology
As I was able to comment in the article related to tendon injuries, there is much controversy about the most accurate term to define tennis elbow. The most common term so far had been ” epicondylitis “, but we have to bear in mind that tendinitis and tendinosis are two conditions that occur at different times in the repair process and therefore need different treatment. Epicondylitis refers to pain in the lateral aspect of the elbow that results from inflammation and micro-rupture of fibers in the extensors of the forearm, something that occurs during the initial symptoms of the process (11).
Various histopathological studies have shown that there is a shortage of inflammatory cells in the tendon tissue of patients with epicondylitis diagnosed several months ago. Alfredson et al. (12) observed normal levels of prostaglandins E2, biochemical markers of inflammation, demonstrating its absence in tendon tissue. These and other studies are aimed at using the term “ lateral elbow tendinosis ” more than “epicondylitis”.
Symptoms
Understanding where and how the tennis elbow process occurs, it is important to identify risk factors and symptoms in order to establish the necessary modifications during physical training.
The main symptom is pain in the lateral aspect of the elbow radiating towards the forearm . It is usually reproduced in activities that involve grip, lifts with a prone grip or those in which you go from a prone grip to a supine one, such as the dumbbell bicep curl (13). Palpation about 5mm distal and anterior to the epicondyle, which is where the extensor carpi radialis brevis originates, also exacerbates the pain (8,11).
Physical examination of the affected arm helps us to observe abnormalities such as muscle atrophy, swelling on the lateral aspect of the elbow, limited range of motion, and / or decreased grip strength compared to the other arm. In addition, pain is often reproduced in activities of daily life such as shaking hands or holding a glass of water, for example.
Anatomical abnormalities can also predispose the athlete to tennis elbow. For example, hyperextension and an increased valgus angle of the elbow, an imbalance between the flexor and extensor muscles of the wrist, and / or a weakness of the forearm muscles involved in grip (2).
On the other hand, there are several tests or functional tests to identify the origin of the injury, as well as the musculoskeletal structures involved, but we are not going to expand on this issue as they must be performed by health professionals such as physiotherapists.

Training modifications
If an athlete meets any characteristic or symptom compatible with tennis elbow, we must adapt the training to their needs, and for this a series of modifications and indications will be necessary, in order not to aggravate the symptoms.
The first thing we must do is reduce the overload to which we submit the tendons on the lateral aspect of the elbow (3). Absolute cessation of activity is not recommended unless the symptoms are very acute and painful. In that case, a rest period will be necessary in which we can perform cardiovascular exercise and train other areas of the body. If this is not the case, it should be known that the activity helps in the repair of damaged tissue, but it is necessary to make some modifications to avoid overloading it.
Another factor to take into account is the type of exercise to be performed during the training routine. As you may already be intuiting, it will be necessary to reduce the volume of those exercises that involve the prone grip of the forearm and traction, such as an inverted bicep curl, as we will only be able to exacerbate the symptoms of the injury (8). We will replace it with a bicep curl with a supine grip so that the force falls on the flexor muscles of the wrist and relieves a little of the extensor muscles, which is the one involved in the tennis elbow.
It will also be convenient to substitute exercises with barbells and dumbbells for exercises on machines , since this way we reduce the load on the muscles involved in the grip, which is overloaded in the exercises with free weight.
In those who practice racket sports we can also make a series of modifications , from a possible change in the hitting technique that may have triggered the injury, to a change in the size of the grip and the weight of the racket, because how much The heavier the racket and the narrower the grip, the more force the wrist extensor muscles will have to exert to control the racket, thereby exacerbating the symptoms. The latter could also be applied to the dumbbells in weight training (11).

Use of elbow or wrist guards
It is estimated that 21% of people diagnosed with tennis elbow are also prescribed the use of elbow or wrist braces (6,14). The wrist brace consists of a splint, and the elbow is usually a strap on the proximal part of the forearm, very close to the elbow. There is much controversy about their efficacy, and below we will detail the scientific evidence surrounding their efficacy.
Wrist braces are, at least the most commonly used, splints made of firm material that keep the wrist in a neutral position and reduce stress on the extensors. So far everything is perfect, however, in a study in which 4614 cases of tennis elbow were reviewed, no benefit was found in those who used a wrist strap compared to those who did not (9). In that same study, they observed 253 workers with this injury, and found that those who used a wrist brace had a greater limitation at work and needed more medical assistance and treatment than those who did not use it.
Elbow pads usually consist of tapes of variable width that are placed compressing the proximal part of the forearm, relieving pressure on the involved extensor muscles of the tennis elbow, and also reducing the force it can generate (15). Groppel and Nirschl observed the electromyographic activity of the wrist extensors during the serve or backhand in a tennis match, and Snyder-Mackler the isometric contraction (15). In both, a decrease in EMG was observed. Knebel et al. (16) found evidence of greater fatigue in the extensor muscles when the elbow was used, weakening the area and facilitating the appearance of secondary complications. Struijs et al. (7) found that elbow pads could be useful to maintain the same levels of activity, but only in the short term and in those with acute pain. Finally, a study by Van De Streek et al. (14) determined that there were no benefits with the use of wrist or elbow pads, neither at the functional level, nor at the level of strength or pain.
Sources:
Christopher M. Kaczmarek. Strength and Conditioning Journal. April 2008.
- Yu, J and Habib, P. Common injuries related to weightlifting: MR imaging perspective. Semin Musculoskeletal Radiol 9: 289–301, 2005.
- Maffulli, N and Wong, J. Types and epidemiology of tendinopathy. Clin Sports Med 22: 675–692, 2003.
- Wilson, J and Best, T. Common overuse tendon problems: A review and recommendation for treatment. Am Family Phys 72: 811–818, 2005.
- Calhoon, G and Fry, A. Injury rates and profiles of elite competitive weightlifters. J Athl Ttrain 34: 232-238, 1999.
- Faes, M, Van Elk, N, De Lint, J, Degens, H, Kooloos, J, and Hopman, M. A dynamic extensor brace reduced electromyographic activity of wrist extensor muscles in patients with lateral epicondylalgia. J Orthop Sports Phys Ther 36: 170–178, 2006.
- Struijs, P, Korthals-De Bos, I, Van Tulder, M, Van Dijk, C, Bouter, L, and Assendelft, W. Cost effectiveness of brace, physiotherapy, or both for treatment of tennis elbow. Br J Sports Med 40: 637–643, 2006.
- Struijs, P, Assendelft, W, Kerkhoffs, G, Souer, S, and Van Dijk, C. The predictive value of the extender grip test for the effectiveness of bracing for tennis elbow. Am J Sports Med 33: 1905–1909, 2005.
- Vicenzino, B. Lateral epicondylalgia: A musculoskeletal physiotherapy perspective. Manual Ther. 8: 66–79, 2003.
- Dereby, V, Devenport, J, Giang, G, and Fogarty, W. The effects of splinting on outcomes for epicondylitis. Arch Phys Med Rehabil 86: 1081-1088, 2005.
- Murphy, K, Giuliani, J, and Freedman, B. Management of lateral epicondylitis in the athlete. Op Tech Sports Med 14: 67–74, 2006.
- Plancher, K, Halbrecht, J, and Lourie, G. Medial and lateral epicondylitis in the athlete. Clin Sports Med 15: 283-305, 1996.
- Alfredson, H, Ljung, BO, Thorsen, K, and Lorentzon, R. In vivo investigation of ECRB tendons with microdialysis technique-no signs of inflammation but high amounts of glutamate in tennis elbow. Acta Orthop Scand 71: 475-479, 2000.
- Levin, D, Nazarian, L, Miller, T, O’Kane, P, Feld, R, Parker, L, and McShane, J. Lateral epicondylitis of the elbow: US findings. Radiology 237: 230–234, 2005.
- Van De Streek, M, Van Der Schans, C, De Greef, M, and Postema K. The effect of a forearm / hand splint compared with anelbow band as a treatment for lateral epicondylitis. Prostethics Orthotics Int 28: 183-189, 2004.
- Anderson, M and Rutt, R. The effects of counterforce bracing on forearm and wrist muscle function. J Orthop Sports Physl Ther 15: 87-91, 1992.
- Knebel, P, Avery, D, Gebhardt, T, Koppenhaver, S, Allison, S, Bryan, J, and Kelly, A. Effects of the forearm support band on wrist extensor muscle fatigue. J Orthop Sports Phys Ther 29: 677–685, 1999.
